Trauma and Beyond specializes in the treatment of Dissociative Identity Disorder (DID) and its subtype of OSDD Type-1, standing out as one of the leading DID treatment centers in California.
Clients with Dissociative Identity Disorder (DID) and OSDD Type-1 are among the most underserved and misunderstood populations in mental health, because existing mental healthcare systems are underequipped to provide effective and attuned care. Many clients live with chronic misdiagnosis, inaccurately labelled with schizophrenia, personality disorders, or psychosis, while the underlying dissociative nature of their experience goes unrecognized.
Research and clinical understanding suggest that DID/OSDD Type-1 most commonly develops when an individual, usually early in childhood, must dissociate from a fundamentally unresolvable internal experience, most frequently extended and severe abuse by someone the child must also love and trust. Dissociation is defined as disconnection in the function of consciousness (thoughts, feelings, memories, sense of self, etc.). When an individual must dissociate extensively for survival, dissociation can become part of how the mind is structured.
One way to understand this type of separation in the mind is the theory of structural dissociation. Structural dissociation happens when those who have survived complex trauma experience division of the personality into different parts, each with its own sense of self to varying degrees, and differing capacities for autonomous action. While Trauma and Beyond uses the term Structural Dissociation, there are many other valid and important ways of describing the experience of having separate parts of the self, often referred to as alters. Other terms and concepts include multiplicity, plurality, living as a system, being many, and many more.
Our team engages in ongoing consultation with subject matter experts, continual staff training, and consistent engagement with best practices in this area, with the goal of creating a California DID and OSDD treatment program truly attuned to the unique treatment needs of those living and healing with multiplicity.
What does treatment for DID/OSDD look like at Trauma and Beyond?
Our approach for treatment is fundamentally relational. This means that while we use many different tools, skills, and modalities, the essential treatment frame is the creation of a supportive, relational space in which the individual’s system is empowered to integrate. We may use strategies like parts mapping and meeting places, but our focus is on increasing internal relationship and connection through whatever approaches each client finds the most helpful.
The main goal in treatment is integration, which we conceptualize as meaning full co-consciousness between all parts of the self. We want to empower each client’s system to overcome amnestic barriers, integrate separated trauma memory in a slow and titrated way, and learn to function as an effective team in daily life. Our therapies aim at the “Three C’s”: Co-Consciousness, Collaboration, and Cooperation.
What stands out about our program is the daily, 90 minute individual therapy sessions. This is the recommended session duration for individuals with structural dissociation, giving additional time and space due to the complexity of the system. We operate with a flexible three phase model of stabilization, processing of traumatic memory, and integration, as recommended by the ISSTD’s treatment guidelines.
What does treatment look like if I’m only able to stay a short time?
For individuals with DID or other forms of structural dissociation, treatment duration does matter. The work cannot move too quickly, or it may overwhelm and destabilize. For individuals who can only stay for shorter durations, we focus on psychoeducation about structural dissociation and on building targeted coping and stabilization skills, such as those found in the Finding Solid Ground program. For work focused on deep integration of traumatic memory and creation of full co-consciousness within the system, we recommend a longer treatment duration. Our Los Angeles based DID treatment program works to provide you with the best possible outcomes for any treatment duration, and our tele-health DID therapy in California helps make treatment more accessible for many clients.
How do you navigate groups for clients with alters/parts?
We utilize a highly flexible approach for groups, working to ensure the group therapy modality is supportive and not harmful. We typically focus on experiential and psychoeducational groups, rather than process groups, for clients with structural dissociation. Our group facilitators are familiar with multiplicity, and will respond supportively if a client switches or blends during group time. Certain groups, such as our art therapy groups, are spaces where younger parts can front and directly engage. In other groups where the structure includes engagement with adult peers in conversation or discussion, younger parts who come forward are gently and kindly invited to color or do another quiet activity during the group time.
Is there pressure to fuse or combine parts during the treatment process?
No, there is not. For some individuals with separate parts or alters, the healing process may include the free choice for multiple parts to combine into one, or into the larger consciousness. This can be referred to as fusion. However, many systems have parts that even once fully healed desire to maintain their independent selfhood. Our goal at Trauma and Beyond is complete self-determination for the client. We support each system member in determining what will truly feel the most supportive for them, and empower the client to settle into a final constellation that feels the best for their unique healing journey.
What if I’m not sure I have DID?
Trauma and Beyond works with many clients who experience internal divisions of the self, and our comprehensive diagnostic and testing process guides each client to the appropriate diagnosis that best explains their lived experience.
We utilize a combination of gentle, supportive clinical interviewing along with outcome measures (The MID 60, DES – II, and full MID if needed) to help collaboratively identify whether a client meets the full criteria for DID, or might have another type of dissociative or trauma-related disorder.
As mentioned above, OSDD Type-1(Other Specified Dissociative Disorder Type-1) also includes a sense of having divisions in the self; it is a type of structural dissociation with fewer amnestic barriers than the full diagnosis of DID. Individuals with the dissociative subtype of PTSD or C-PTSD may feel different parts internally as well, but more congruently with ego-states than structurally separate parts. Our team helps differentiate between these experiences.
We hold space for the complexities of the diagnostic process. For certain clients, the fear of what the diagnosis might mean can impair assessment, and intense anxiety may occur when discussing or exploring internal experiences. We are also sensitive to the complex role that social media plays. It helps provide much needed recognition and space for community around these experiences, but may also lead to some confusion around the diagnostic picture. We balance all these complexities with the awareness that DID is historically and significantly underdiagnosed, and we approach each client’s experience with full openness.
Our team is trained to work compassionately towards the most accurate diagnosis for all our clients. We avoid overdiagnosis through careful testing, and treat the diagnostic process with gentleness and support for clients who may be very anxious about exploring this area of their lives and selves.
Are you open to approaches outside of Structural Dissociation Theory?
Absolutely. Our team is trained in Structural Dissociation Therapy, and you’ll notice we use a lot of that language and framework. However, we are deeply aware that multiplicity remains a highly nuanced, individualized experience, and there are many other ways to approach and understand it. Our team is prepared to work within whatever framework you utilize to understand your experience of multiplicity, as our goal is to encourage the understanding that feels the most healing and empowering for each individual.
Information about DID and OSDD Type-1 for Loved Ones and Support Individuals
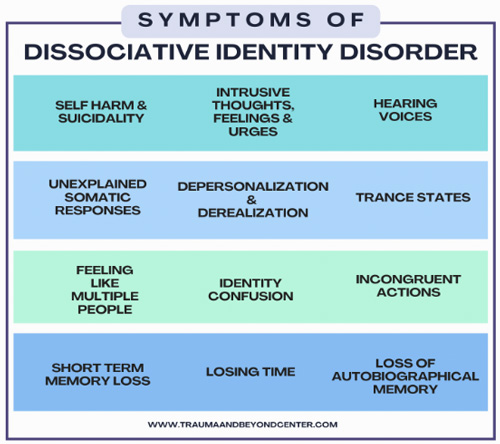
The infographic and FAQ shown below are tools to help individuals who live with DID or OSDD Type-1 and their loved ones understand and communicate about the experience.
Our team at Trauma and Beyond provides Dissociative Identity Disorder therapy in Los Angeles and throughout California via tele-health, and this can include family sessions. We provide psychoeducation and conjoint sessions to loved ones to help them understand the client’s experience, although only to support individuals who are safe, appropriate, and not involved in any history of severe abuse. We believe that those living and healing with multiplicity thrive when supportive, informed support individuals are part of the healing process. We offer these resources to help empower clients and families to talk openly about living and healing with dissociative disorders.
Infographic: Symptoms of Dissociative Identity Disorder
DID and OSDD Frequently Asked Questions (FAQ)
Is there a part that is the “Real” person?
No, some systems have a majority stakeholder in the personality, but others do not. Either way, the “Real” person is the totality of who they are, all parts included! Individuals may have parts that tend to engage with daily life, and parts who are more focused on trauma. The daily life parts may be present more frequently to outside observers, but it does not make them more “Real” than trauma facing parts.
Does the person know they have parts?
Often, no! People with parts feel very confused about what is happening to them, and can become scared, embarrassed, and agitated when they notice evidence parts are present. It’s important to not become frustrated if an individual with parts seems unaware of the presence or impact of parts, as they may genuinely not be.
Do people sometimes make up having parts?
While there is more concern about inaccurate self-diagnoses in recent years due to certain types of social media content about DID, individuals with truly separate parts are not making it up. Having parts is not a choice, and is best understood as a courageous way of adapting to survive extreme suffering.
Are parts scary?
No. Misleading horror movies and media content can cause a lot of shame and stigma by showing parts as frightening. While some parts may express themselves as angry, sound scary, or even do things to hurt the body, it is always from a place of pain. Parts are not inherently wrong or bad, and should not be treated as such. All parts can heal, and all parts are a valued part of who the person is.
What is “Switching”?
Sometimes, the part that is “Fronting” changes, with a new part coming forward in the person’s consciousness. It can be very clear, or very subtle. Parts can also “Blend,” where they partially come forward, or send emotions, body sensations, or memories without coming forward at all. When someone is able to heal, there is less full switching, and more organic transition between parts, without loss of time or memory.
What does getting better look like for someone with parts?
Some parts may choose to “Fuse,” become one, but many may not. Getting better means all parts can communicate, work as a team, and heal from their collective trauma. It’s important to support each person in whatever internal arrangement feels the best for them.
Where can I learn more about this?
You can check out the following resources for more information about DID/OSDD Type-1, both for those with lived experience and for their support individuals. The following websites represent a combination of professional sources and, most importantly, voices of lived experience.
Lived experience voices:
Professional voices: